

Vitamin D Looks Powerful, Underutilized for COVID-19
Early data justifies urgent wider testing & widespread use until then
May 6, 2020 Karl Pfleger, karl@agingbiotech.info
Vitamin D is safe, cheap, and widely available, but deficiency is common and well known to be a widespread health problem, including worsening viral & lung risks. It’s been considered possibly helpful against COVID-19, but recent data suggests the benefit might be very large. Perhaps as important & easy as face masks? As effective as remdesivir? Experts urgently call for more data & possible widespread use. I summarize the evidence to increase awareness by the public & policymakers in case doing so might save lives or hasten the end of the crisis.
10-point summary and table of contents:
Vitamin D facts from before COVID-19
1. D status associates w/ all-cause mortality
2. Low D causes many health issues including viral & lung related
3. D extends lifespan of nematodes by slowing an aspect of aging
4. D deficiency is widespread & long labeled a pandemic by some
5. Older adults are not more deficient than younger adults
6. Moderate D supplementation has low risk
7. Blood tests for D level are easy, cheap, and widely available
COVID-19 vit-D related biology, data, & implications
8. Biological arguments suggest D usefulness for COVID-19
9. COVID-19 case severity associated with low D status
10. COVID-19 fatality strongly associated with low D status
Correlational data supported by many pieces of causal evidence
Author info, disclaimers, and conflicts of interest
Note: This is not meant to be an academic review article. Every effort has been made to be correct on each point, but due to the urgency of the situation, I have favored speed of dissemination over comprehensive references. The goal is to piece together disparate data to paint the most coherent and helpful picture possible at the moment and to provide jumping off points for deeper analysis and context for incorporating future new information. Feedback or corrections welcomed. Linked references inline rather than at the end.
Vitamin D facts from before COVID-19
Two threshold values are commonly applied to vitamin D blood levels: 20ng/ml (50nmol/L) and 30ng/ml (75nmol/L) with common terminology creating 3 buckets of D status: deficiency at <20nglml, insufficiency at 20-30, and sufficiency/normal at >30.
1. D status associates w/ all-cause mortality
This is a representcative reverse-J shaped plot of mortality risk vs. D level. For many similar plots and links to studies, do a web image search for: vitamin d mortality. The above here is from a big study whose results are broadly representative: Gaksch et al, “Vitamin D and mortality…” PLOS ONE, 2017, which tracked 26,916 people for median 10.5 years during which 6,802 died. Note that risk begins to rise below the insufficiency level and rises sharply below the deficiency threshold, but risk rises only slowly and not statistically significantly for high levels. In other words, the risk from having too little vitamin D is high but the risk from too much vitamin D is low.
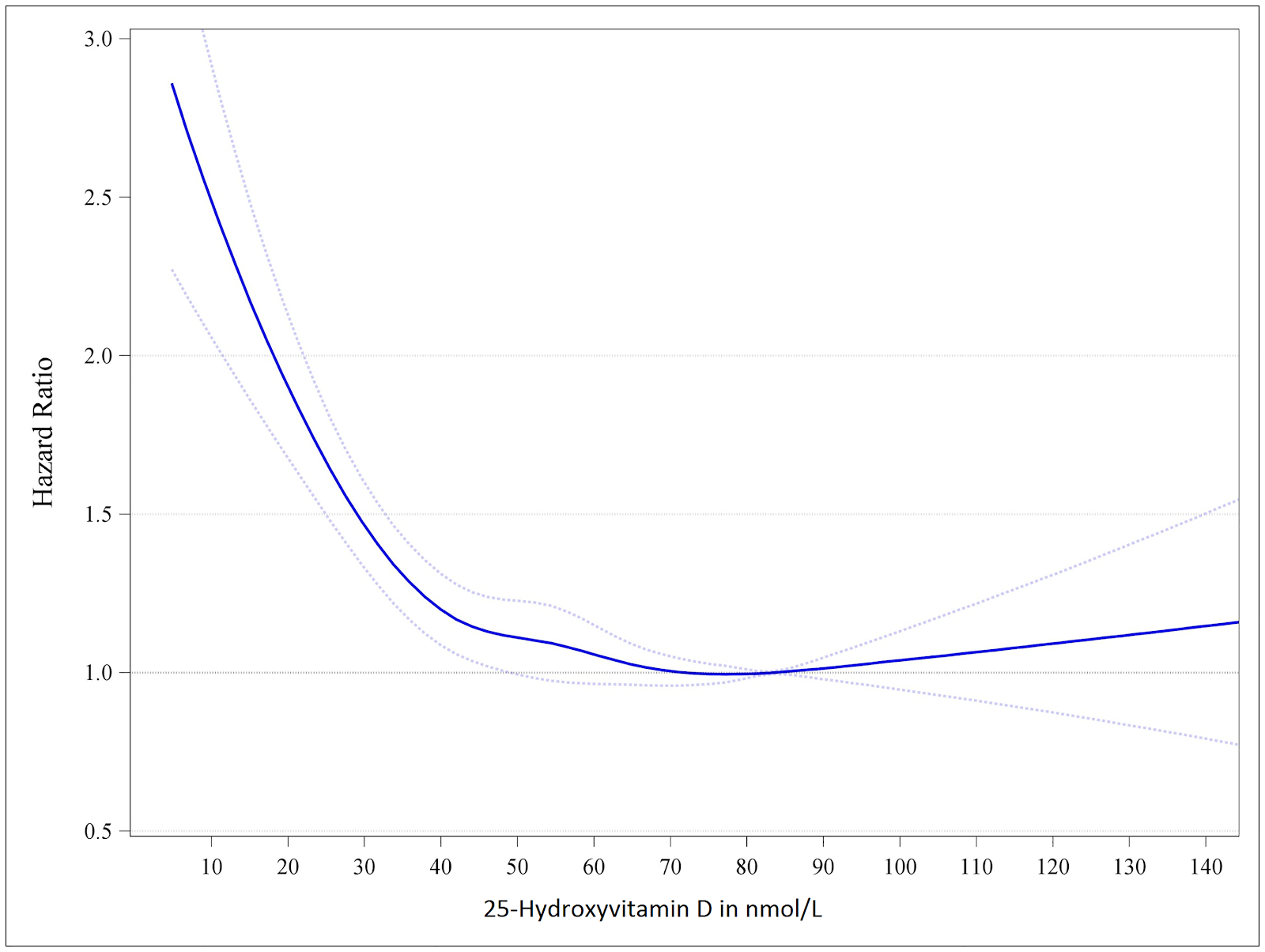
Chowdhury et al, “Vitamin D and risk of cause specific death…” BMJ, 2014 concluded that 13% of US deaths were attributable to low vitamin D, vs. 20% for smoking, 11% for physical inactivity, and 9% for alcohol.
2. Low D causes many health issues including viral & lung related
Vitamin D is perhaps best known for regulating calcium metabolism with deficiency related to bone disorders, such as osteoporosis. But deficiency is also implicated in many other diseases, especially most of the top chronic diseases of aging, including cancer, cardiovascular disease (CVD), diabetes, and neurodegenerative diseases such as Alzheimer’s. Literature is easy to find. Wang et al, “Vitamin D and chronic diseases” Aging Dis., 2017 is a good example. Low D is also implicated in varied other diseases including depression (see the just mentioned paper) and erectile dysfunction (see Talib et al, “The role of vitamin D supplementation on erectile function” Truk J Urol., 2017, which shows that D may play a role in this pathology in ways other than just its effect on the vascular system).
Vitamin D has been long known to affect both the immune system and consequently risk of infectious disease. This point is not controversial and literature is easy to find by searching for vitamin D and immune or infection. For example, Gunville et al, “The role of vitamin D in prevention and treatment of infection” Inflamm Allergy Drug Targets, 2013.
In particular, vitamin D can be beneficial with regard to pulmonary (lung) problems. As the above paper states, “vitamin D deficiency is associated with increased risk and greater severity of infection, particularly of the respiratory tract.” Yang et al, “Effect of vitamin D on ACE2…” Chinese J Emergency Med 2016 or Xu et al, “Vitamin D alleviates…” Molecular Med Rep 2017 report on experiments (in rats) showing that vitamin D mitigates the effect of acute lung injury by increasing the expression of ACE2, a member of the renin‑angiotensin system (RAS). This will be important later in discussing COVID-19, but was known years ago.
Perhaps the most comprehensive review of vitamin D on varied health problems in humans is ConsumerLab.com, “Vitamin D Supplements Review” report, 2019 (updated 2020), a report that requires a $25 fee to view for 30 days or a website membership currently costing $48/year. ConsumerLab.com conducts lab tests of supplements from varied vendors to insure correct dosing and absence of toxins, but its reports of its lab results also contain very comprehensive literature reviews. [I have no affiliation other than as a customer.] This vitamin D report summarizes human studies on bone/fractures, muscle/balance/falls, vertigo, incontinence, back pain, arthritis, CVD, diabetes, inflammation, asthma, allergies, chronic obstructive pulmonary disease, allergies, dementias, depression, headaches, cancer, colds/flu/respiratory-infections, and several other conditions. A summary of the studies on infectious diseases is that supplemental vitamin D appears to reduce risk the most when patients do not already have sufficient levels and when dosing is daily rather than in periodic large doses, such as once/month.
Many of the studies reviewed by the above sources present epidemiological (associative) data but there are also many randomized controlled trials (RCTs) demonstrating a causal relationship, in addition to the ACE2 work in rats clearly establishing causality in that context.
3. D extends lifespan of nematodes by slowing an aspect of aging
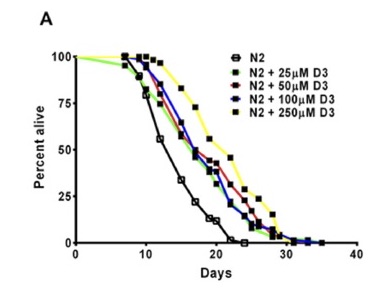
The survival curve above, from Mark et al, “Vitamin D promotes protein homeostasis and longevity…” Cell Reports, 2016, shows that increasing doses of vitamin D extend the lifespan of C. elegans roundworms, a common organism used in studies of aging. This species has no bone, so this work also shows that vitamin D has other effects besides those it is best known for. The paper showed that vitamin D slowed an important molecular aspect of aging related to protein misfolding, a problem that plays a big role in many human age-related chronic diseases such as Alzheimer’s & Parkinson’s disease and other neurodegenerative diseases. Another interpretation is that low vitamin D causes faster molecular aging.
Quantifying the degree of life extension was not the main purpose of this paper but the degree of lifespan extension was reported as 33% in popular-press article (eg, 1, 2), quoting Gordon Lithgow who leads the lab that did the work, and this paper references earlier work showing 39% extension. Note that increasing benefit was seen up to the highest dose used.
4. D deficiency is widespread & long labeled a pandemic by some
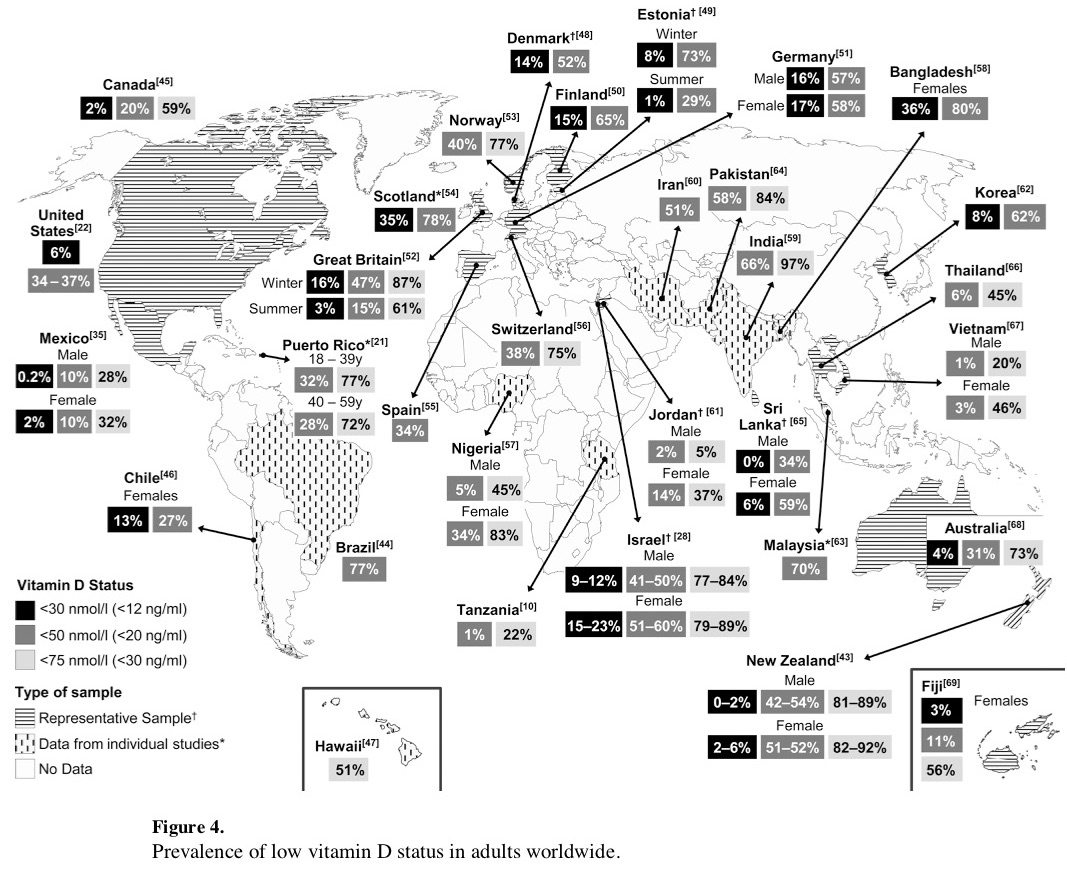
From Palacios et al, “Is Vitamin D deficiency a major global public health problem?”, J Steroid Biochem Mol Bio, 2014. This shows high levels of deficiency or insufficiency across the world.
Multiple authors have labeled vitamin D deficiency itself as a pandemic long before COVID-19. Search scholar.google.com for: vitamin d pandemic. Eg, Holick, “The vitamin D deficiency pandemic…”, Reviews in Endocrine and Metabolic Disorders, 2017.
The chart above shows 34-37% of US adults as deficient. NHANES data from 2005-2006 and from 2011-2012 both suggest the deficiency % is ~40%. For that and more breakdowns by subpopulations, see Parva et al, “Prevalence of Vitamin D Deficiency…”, Cureus, 2018. As in the countries above with data on insufficiency, insufficiency % (mildly low D) should be much higher than outright deficiency, covering much more than a majority of the population. Eg, Australia 73%, Great Britain 61% in summer and 87% in winter.
5. Older adults are not more deficient than younger adults
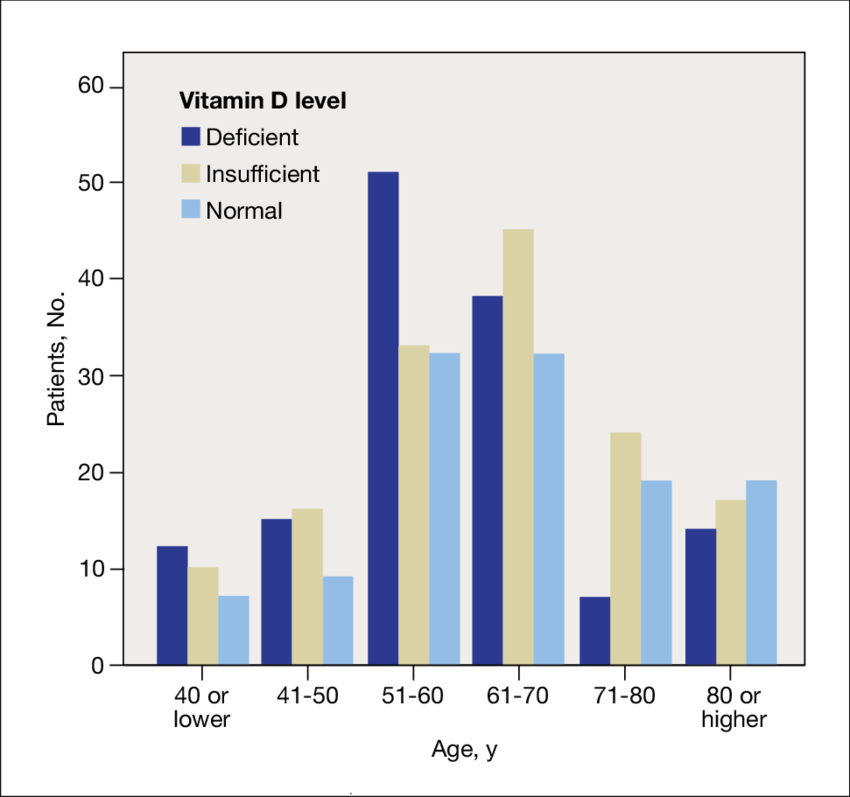
The above chart from Maloney et al, “A retrospective study of serum vitamin D levels in veterans” Federal Practitioner, 2011 shows lower risk of deficiency among the old vs. younger adults. The NHANES data in Parva et al, “Prevalence of Vitamin D Deficiency…”, Cureus, 2018 also showed that those aged >65 had lower prevalence of deficiency than younger adults. Further, Kweder et al, “Vitamin D deficiency in elderly…” Avicenna J Med, 2018 showed no relationship between vitamin D status and age between those aged 75-84 vs. >84, showing that even in the older old there is no consistent pattern of increased deficiency with increased age.
Some discussions, especially in the context of COVID-19, make the point that the old are more at risk of vitamin D deficiency, but that wasn’t what the data seemed to show for targeted queries directly on the question, outside the context of COVID-19. If there is more debate on the subject than the above links show, it was not apparent on first glance, but this document does not try to go deep on this question.
6. Moderate D supplementation has low risk
While it is easy to find lists of conditions that can be caused by too much vitamin D, it is harder to find clear data on what blood levels or D supplementation intake levels trigger any of these problems. One healthline.com webpage suggests that, “toxicity isn’t common and occurs almost exclusively in people who take long-term, high-dose supplements without monitoring their blood levels.” The same article notes that the vitamin D council recommends blood levels of 40-80ng/ml and says that over 100ng/ml may be harmful. The tolerable upper limit of intake for vitamin D is 4000IU (100mcg). There seems to be little data suggesting high likelihood of severe problems at blood levels below 80ng/ml or intakes below 4000IU.
Hypercalcemia is the most commonly cited problem of too much D, but Tebben et al, “Vitamin D mediated hypercalcemia…” Endocr Rev, 2016 says that some patients have blood levels over 80ng/ml without the condition and >80ng/ml is generally needed at minimum, with levels typically severalfold higher to cause symptomatic hypercalcemia. ConsumerLab.com’s report says that this condition is unlike with intakes less than 10,000IU/day.
LifeExtension.com warns that D levels above 100ng/ml were associated with increased risk of atrial fibrillation. This page also notes as people age their body makes and absorbs less D and for example a 70 year old might need to supplement 5000-7000IU/day to achieve blood level of 50ng/ml.
The other most commonly discussed risk of too much D is increased risk of falls in the elderly. Paradoxically, fall risk is also higher with too little D, and the right level of supplementation for minimizing fall risk in the elderly is a matter of debate in the literature. Papers are easy to find with web or literature searches for: vitamin D falls. The notable pessimistic recent paper is Bischoff-Ferrari et al, “Monthly high-dose vitamin D…” JAMA Internal Medicine, 2016, which found a 15% higher risk of falls in those aged 70+ who had had a prior fall in the past year who were given 60,000IU monthly vs. 24,000IU. These doses are equivalent to 2000 or 800 IU daily and only achieved average blood levels well below the high levels mentioned above, but the doses were given in a single large dose once/month, and some authors have suggested that the periodic super-high dosing may be responsible for the increased fall risk. It is also not clear whether this risk would generalize to those younger or those at less risk of falls in the first place (eg, who had not had a prior fall). Lastly, exercise or fall prevention programs can reduce the risk of falls by much more than this increase, eg by half, and thus seems like a good idea for anyone at risk of falls.
ConsumerLab.com’s report echoes the caution about periodic high dosing vs daily dosing noting several studies with negative effects that used periodic high doses. Across all health conditions considered in this report, there were several cases where increasing D levels above 40ng/ml (100nmol/l) began to have negative effects. The report recommends remaining under 40ng/ml. This was the minimum of the optimal range recommended above. This conflict can possibly be explained by the difference between outright toxicity, a more severe problem, vs. mildly worse long-term outcomes for some conditions. Also, it’s likely that some conditions and some studies suggest conflicting optimum ranges.
To summarize what seems most clear, daily vitamin D supplementation at low-moderate doses appears to have very low risk, certainly for blood levels under 40ng/ml. Risk above this level does not start to rise steeply until significantly higher levels. This is broadly consistent with the reverse-J shaped curve for all-cause mortality.
7. Blood tests for D level are easy, cheap, and widely available
Blood tests for vitamin D are common, cheap, and routine. In the US, both LabCorp and Quest provide them. Doctors frequently order them and consumers can order them directly through most of the direct-to-consumer blood test website vendors, for $35-90, including RequestATest.com, WalkInLab.com, DirectLabs.com, PrivateMDLabs.com, and LifeExtension.com. The lowest priced direct-to-consumer test currently costs $35, on sale from $47, from LifeExtension.com using LabCorp.
There are also home finger-prick (then mail away) vitamin D tests, such as from EveryWell.com (currently $79). I have not researched the accuracy of at-home finger-prick tests.
COVID-19 vit-D related biology, data, & implications
Recent papers explain biological mechanisms by which vitamin D may help fight COVID-19 and argue for its investigation or use on that basis, and recent studies show a strong correlation between vitamin D status and COVID-19 case severity. Since the COVID-19 pandemic is so new, most papers specifically about COVID-19 are preprints that have not yet been peer reviewed, which takes considerable time. Thus, individual pieces of information may be suspect and one should look for patterns that are consistent with the other pre-print material and also with the pre-COVID-19 facts from the prior section.
8. Biological arguments suggest D usefulness for COVID-19
Several authors make convincing cases that vitamin D should be helpful against COVID-19 based on biological arguments, both molecular and based on infectious disease literature, as well as other circumstantial evidence. One of the most notable molecular biological connections is that COVID-19 affects the renin–angiotensin system (RAS), especially expression of a gene called ACE2, and vitamin D corrects these effects. This document will not try to summarize the relevant molecular biology in any greater detail. The papers in this section provide good jumping off points for further study.
Grant et al, “Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths” Nutrients, 2020 broadly reviews evidence for D to help with infectious diseases, pneumonia, and inflammatory cytokines that damage the lungs and discusses some of the aspects of COVID-19 infection that are known to relate to things known to be also relevant to vitamin D. The paper also considers circumstantial evidence such as timing and latitude of COVID-19 outbreaks before going so far as to recommend that those at risk of influenza or COVID-19 consider taking 10,000IU/day of vitamin D (D3) for a few weeks to rapidly raise levels followed by 5000IU/day with the goal to raise blood levels to or above 40-60ng/ml, finally suggesting that higher doses might be useful for those with active COVID-19 infection.
Ghavideldarestani et al, “Role of vitamin D in pathogenesis and severity of COVID-19 infection”, Preprint.org, 2020 considers many aspects of the biology of vitamin D and COVID-19, notably including ACE2 & RAS, before concluding that D may be specifically helpful against COVID-19.
Davies et al, “COVID-19 and vitamin D information” working papert, 2020 (which claims “This document is for medical professionals only”) also considers the details of ACE2 & RAS. In addition, it notes that severe COVID-19 outbreaks and most deaths have occurred north of 20 degrees latitude (as of late March, 2020). The authors call for more vitamin D blood testing.
9. COVID-19 case severity associated with low D status
Alipio, “Vitamin D supplementation could possibly improve clinical outcomes of patients infected with coronavirus-2019 (COVID-19)” SSRN, 2020 examined 212 cases of COVID-19 in 3 hospitals in Southern Asia with vitamin D status. Cases were split by severity into mild, ordinary, severe, & critical. D status was split into deficient, insufficient, & normal. A clear pattern of increased case severity with lower D level is evident from the basic descriptive statistics:
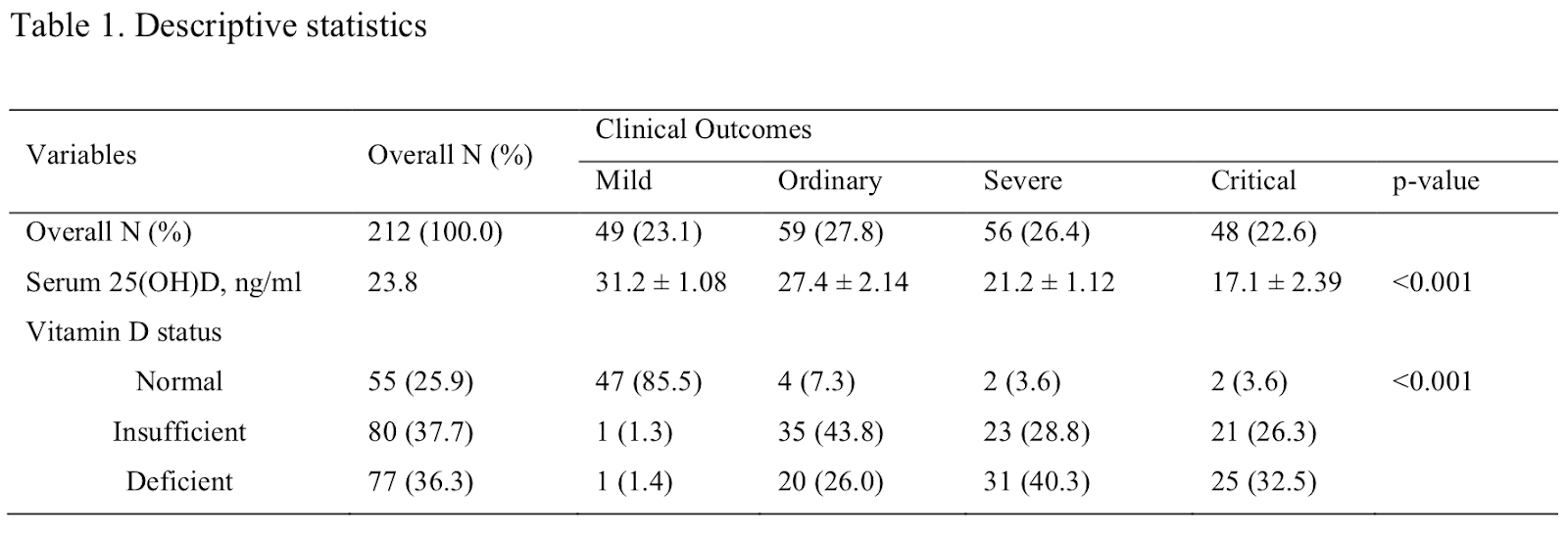
A multinomial logistic regression reinforced that lower D was associated with more severe cases. Notable from the simple statistics: Of the cases with normal D levels, 47 of 55 (85%) were the mildest category and only 2 of 55 (3.6%) were critical. Of the critical cases, only 2 of 48 (4.2%) had normal D. Of mild cases, only 1 out of 49 had deficient D and 1 had insufficient, so only 2 out of 49 (4.1%) had lower-than-normal D. This is a strong association.
Of note, the hospitals tested D levels repeatedly and also had pre-admission levels. The author performed an analysis to determine whether the levels changed much within a patient and found that they did not for 95% of the overall cases examined, which then made up the 212 cases kept for analysis. The vitamin D levels used were pre-admission. Thus, though the data are associative, the reverse causality that the infection caused dropping D levels can be ruled out.
A smaller study of just 20 people in 1 care facility, Lau et al, “Vitamin D Insufficiency is prevalent in severe COVID-19”, medRxiv, 2020, report the same basic association. 13 of 20 patients required ICU admission. “The baseline prevalence of VDI [Vitamin D Insufficiency] amongst ICU patients is 30-40%. In this study, we found that 84.6% [11 out of 13] of COVID-19 ICU patients had VDI, vs. 57.1% of floor patients.” What’s more, “Strikingly, 100% of ICU patients less than 75 years old [11 out of 11] had VDI.” Of these, 65% had outright deficiency below the lower 20ng/ml level.
10. COVID-19 fatality strongly associated with low D status
Raharusun et al, “Patterns of COVID-19 mortality and vitamin D: An Indonesian study” SSRN, 2020, using a cohort of 780 patients, showed (after correcting for age, sex, & comorbidities) that patients with D insufficiency were 7.6x likelier to have died than those with normal D. D deficient cases were 10x likelier to have died. The above studies did not attempt to control for possible 3rd hidden variables that could have caused the association between D level and case severity. This study is notably different (a) because it did that for the 3 most obvious other factors, age, sex, & co-morbidities, (b) due to the much larger size of the cohort, and (c) because it includes outright fatality data.
The univariate analysis that didn’t correct for the above factors showed 12.5x & 19x high risks of dying for insufficiency & deficiency respectively, suggesting that males, the older, & those with co-morbidities probably had worse D levels in this cohort. The adjusted numbers above are thus more appropriate, but the raw numbers are compellingly stark:
177 out of 179 D-deficient patients (98.9%) died.
187 out of 213 D-insufficient patients (88%) died.
16 out of 388 D-sufficient patients (4%) died.
The overall fatality rate of 49% (380/780) seems high relative to official Case Fatality Rates for all confirmed cases in most geographies reporting them, but the paper specifies its data comes from Indonesian government hospital records, implying without clearly saying that the subjects were hospitalized. CFR of hospitalized patients should be expected to be higher than total CFR. CFR given hospitalization is not commonly reported and probably varies considerably by place.
The strength of the relationship demonstrated above is remarkable. This is just one not-yet-peer-reviewed study from one geographic area, so the results may not be reproducible, but to the extent that they are representative of the wider relationship they represent a staggeringly compelling call to action.
Discussion
Even before COVID-19, given the low cost & wide availability of vitamin D tests, the widespread deficiency, and the health & mortality consequences of such deficiency, and the low risk of supplementation, it is surprising that more patients and doctors don’t test and intervene to raise D levels. New data arising in the context of the global COVID-19 pandemic, which is both a health & economic crisis, make the case look even more lopsided. Any small risk from short-term, conservative increase in D levels is likely heavily outweighed by experted (in the statistical sense) short-term benefit against the pandemic, even if that expected benefit is not a guarantee but rather a much less than 100% chance of a big benefit, as implied by above data.
Correlational data supported by many pieces of causal evidence
Correlational data is often criticized and it is true that it is not as good as equivalently sized Randomized Controlled Trials (RCTs), but criticism of correlational data often goes too far. Correlational data has value, especially if it is part of a coherent collection of varied evidence.
The association between D levels and all-cause mortality (§1), some of the associations with health issues (§2), and the associations with COVID-19 case severity (§9-10) are correlational. But much of the rest of the evidence suggests a causally protective effect for vitamin D against COVID-19:
- Much existing knowledge about vitamin D and health is causal, from many RCTs (§2).
- Vitamin D causally affects lifespan, or equivalently rate of aging (§3).
- §5 and §10 explicitly remove age, sex, and comorbidities as alternative explanations.
- The lack of decreasing D during infection in §9 argues against the reverse causation.
- And finally, the biological arguments (§8) explain some potential causal mechanisms.
It’s important to note that none of the papers in the COVID-19 section above have any declared conflicts of interest, nor probably any of the references anywhere in this document. Indeed, it’s hard to imagine how anyone could substantially profit from vitamin D. This contrasts with several other COVID-19 related efforts currently underway.
Urgent, important questions
What is the actual prevalence in the population of hospitalization-severity cases in young and middle-aged adults with sufficient vitamin D levels? This has important implications for who needs to continue to shelter-in-place and how quickly the majority of the working-age-population can return to full productivity. The above data do not show conclusively but do suggest the possibility that a large fraction of the non-old who succumb may be D deficient.
How much lower would widespread D sufficiency make overall COVID-19 Infection Fatality Rate (IFR)—the % chance of fatality given infection? How much would it correspondingly lower the chance of hospitalization and chance of permanent damage (eg, long-term lung damage) given infection, not to mention the chance of spreading the infection? There is less data available on baseline levels of these latter risk percentages, especially the last. The hospitalization question is important in estimating any intervention’s potential to reduce hospital demand exceeding capacity in the future. The chance of spread, eg: change in R0, question is important for estimating how any intervention could accelerate the easing of distancing restrictions and economic closures without causing further outbreaks. But the IFR is probably the easiest thing to estimate despite the already considerable difficulties and controversy in estimating both total cases and total deaths, both of which have been much in the news in April-May, 2020.
Covering the topic of COVID-19 IFR is beyond the scope of this document, but very briefly, Streeck et al, “Infection fatality rate of SARS-CoV-2…” preprint, 2020 recently provided one of the best estimates of IFR from Germany, estimating it to be 0.4% [0.3-0.5%]. This study used a less problematic sampling methodology than earlier studies. For comparison, influenza IFR is about 0.04%.
If we optimistically assume the Raharusun et al’s Indonesian study numbers are representative and capture a fully causal D level to case severity relationship, and we simplistically reduce the raw death numbers for each D level by their corrected model’s multipliers (7.6x, 10x) as if an intervention had boosted those patient’s D levels to sufficiency, we would reduce the 177+187+16=380 total deaths to 17.7+24.6+16=58.3, a 6.5x reduction (15% of the deaths that would happen without the intervention). This simplistic back-of-the-envelope calculation may be useful to think about as an upper bound on potential benefit from vitamin D intervention. Though in other ways even this number is conservative since for example the deficiency and insufficiency prevalences in the US are higher than for the patients studied in Indonesia (US deficiency is ~40% vs. 23% in this study).
Did one of these 3 new studies make a spreadsheet error somewhere? The fact that 3 studies came up with broadly consistent patterns makes this seem less likely, or even if it did happen, the pattern may still hold. Even if further review of the above studies or newer, better data shows reduced benefit, the magnitude of potential benefit currently looks so large that the reduction would have to be massive to reduce it to an unhelpful level. Roughly 5,000 people globally die per day of COVID-19. If vitamin D could reduce that by 6x, 5x, 4x, 3x, or even just 2x it would save tens of thousands per week.
Immediate recommendations
One thing absolutely clear is that hospitals & doctors should get and share vitamin D blood tests for those with suspected or confirmed COVID-19 cases as soon as possible. The US is still seeing tens of thousands of new confirmed cases/day, with almost 100,000/day worldwide. Testing just a tiny fraction of past or current cases would be a flood of useful data. Looking for cases in which the final outcome is already known and for which D status was measured would be especially helpful, as would widespread aggregation of this data.
The change.org petition “We Call for Open Anonymized Medical Data on COVID-19 and Aging-Related Risk Factors” proposes opening up a wide variety of data related and should be considered carefully by those in positions to increase open access to such data. Everyone else should consider signing.
In addition to correcting for age, sex, and co-morbidities, future analyses should also attempt to take ethnicity and obesity into account since they are known to correlate with both COVID-19 severity and vitamin D status.
Groups at higher COVID-19 risk (the old, those with comorbidities, front-line healthcare workers, and possibly all males) should particularly consider having their vitamin D status checked and/or taking at least a conservative supplement dose if not doing so already, at least until additional data become available. Note that ConsumerLab.com’s report says each 1ng/ml increase in blood level requires roughly an additional 100IU/day intake (double if obese), and it can take 6 weeks to reach the new level.
There are currently 7 trials registered on ClinicalTrials.gov to investigate vitamin D as an intervention for COVID-19. 3 of these have estimated completion dates of June 30 through July 2020 and the rest not until Dec 2020 or later. RCTs are of course the gold standard for quality causal data, but RCTs are ethically problematic when sufficient evidence exists that any group of participants is likely to have dramatically worse outcomes. The results of the NIH remdesivir trial were published ahead of peer review partially out of ethical concerns in the context of only a weak, mildly different length of hospital stay. Those running clinical trials of D for COVID-19 need to carefully monitor new evidence on D as it comes out and repeatedly consider the ethics of continuing control arms. Even based on only current data, keeping any controls D deficient for the length of the study seems ethically questionable.
Conclusion
The ease and extreme low cost of acquiring additional data on vitamin D in the context of COVID-19 (which is essentially zero relative to the other costs of the crisis) makes such acquisition an imperative. It could also be accomplished very quickly.
Until then, there is insufficient evidence to conclude that vitamin D is a magic bullet against COVID-19. It absolutely cannot be concluded at this time that it can take the place of masks or allow for faster easing of distancing or sheltering restrictions. However, it is compatible with current information that vitamin D could play an important role in future easing of restrictions prior to availability of a vaccine, if the relationship between D status and infection severity holds.
In the meantime, unlike new pharmaceuticals or repurposed use of existing drugs, in which new data on efficacy are absolutely necessary, decades of good science suggest that the risk of utilizing vitamin D against COVID-19 is low, perhaps even negative given the global public health problem that vitamin D deficiency already was before COVID-19. And the best available current data suggests that the risk of underutilizing vitamin D in the current crisis is high.
Author info, disclaimers, and conflicts of interest
I am not a doctor nor a public health or government official, and nothing in this document constitutes medical advice. Look at the data yourself, talk to medical professionals, and draw your own conclusions.
I do have a PhD from Stanford in a data science area (machine learning & AI) and a decade of work experience at Google doing data analysis and related activities. I have followed the science of nutrition and lifestyle’s effects on long-term health for 2 decades, and I now work in biotech. So I have some experience looking at varied data sources, reading academic literature, and understanding some aspects of biology, FWIW.
I have no conflicts of interest to declare.
This document grew out of some brief posts I made on social media in response to recent papers. When I looked at the details of the data on the strength of the relationship between vitamin D and COVID-19 case severity, and considered the context of everything known about vitamin D including aging and its relationship to COVID-19, I became worried that humanity might be failing to utilize a powerful tool to save lives and help end the crisis.
Thanks to Uri Lerner, Eric Uhrhane, and Michael Angelo for feedback.

